MR imaging is the most accurate technique for the evaluation of GP,
and MR cholangiopancreatography (MRCP) is the primary imaging modality for the visualization of the pancreatic and biliary ducts in GP.
This entity presents a variety of MR imaging appearances which include sheet-like mass appearance,
inflammatory changes,
groove cyst lesions,
duodenal wall thickening and duodenal stenosis,
common bile duct tapering,
pancreatic duct morphology,
widening of the space between the distal pancreatic and common bile ducts and duodenal lumen on MR cholangiopancreatography and banana-shaped gallbladder.
MASS IN THE PANCREATICODUODENAL GROOVE
The most typical presentation of GP on MR imaging is a sheet-like mass between the head of pancreas and the C-loop of duodenum.
This mass is usually hypointense to pancreatic parenchyma on T1-weighted images (Figure 2),
and can be isointense or slightly hyperintense relative to the pancreas on T2-weighted images (Figure 3).
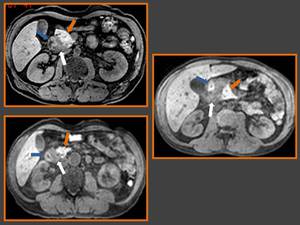
Fig. 2: Axial fat-suppressed T1-weighted MR images show three images of different degrees of sheet-like mass appearance (white arrows) of groove pancreatitis, duodenum (blue arrow) and normal pancreas (orange arrow).
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
This variation in the T2 signal has been related to the duration of the disease,
since subacute disease exhibits brighter T2 signal due to edema (Figure 3),
and chronic disease has lower signal because of fibrosis.

Fig. 3: Axial T2-weighted image reveal in the pancreaticoduodenal groove a sheet-like mass appearance with a predominant slightly hyperintense signal (white arrows) relative to the pancreas (orange arrow) and a anterior and smaller hypointense portion (green arrow). Duodenal wall thickening (blue arrow) and small cyst (yellow arrow) can also be seen.
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
Contrast-enhanced dynamic images show a delayed and progressive inhomogeneous enhancement.
Delayed enhancement may also be seen in the thickened duodenal wall.
These dynamic imaging features reflect the fibrous nature of GP lesions.
It is important to keep in mind that this type of presentation of GP,
especially the segmental form,
should be considered in the differential diagnosis with pancreatic adenocarcinoma (PA).
Imaging characteristics of these two entities may overlap considerably,
because PA is a relatively hypovascular lesion with dense fibrotic tissue,
so the contrast enhancement patterns can be similar in both lesions.
A key point for this differentiation is the presence of vascular invasion in cancer,
which usually has a more round and discrete appearance and is associated with an abrupt irregular ductal stricture.
INFLAMMATORY CHANGES
In this form of presentation,
hypointensity of the pancreatic head or the entire gland on T1-weighted images is seen (Figure 4 A),
commonly associated with parenchymal atrophy and ductal dilatation (Figure 4 B and 4 C).
These aspects reflect the chronicity of this inflammatory disease,
with progressive loss of glandular cells,
protein,
and lipidic contents of the gland,
which are substituted by fibrous tissue.
Enlargement of the pancreatic head may be present.
In the GP pure form the pancreas is spared showing the usual bright T1 signal intensity.

Fig. 4: (A) Axial fat-suppressed T1-weighted MR image show hypointensity of the pancreatic head (white arrow) with volume loss of pancreatic parenchymal (orange arrows) and main pancreatic duct dilatation (green asterisks), frequent on chronic pancreatitis, also seen in (B) axial T2-weighted image. (C) Coronal thick-slab MR cholangiopancreatography image shows main pancreatic duct dilatation (orange arrows) with multiple dilated side branches and common bile duct tapering (green arrow), which are typical of chronic pancreatitis, and cysts in the pancreaticoduodenal groove (blue arrows).
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
GROOVE CYSTS
Cystic lesions are in most cases seen in the groove area and/or in the duodenal wall,
with high signal intensity on T2-weighted images.
MR cholangiopancreatography (MRCP) is helpful in showing the relationship between the ductal system and the cystic changes (Figure 4,
5,
6, 8 and 10).

Fig. 5: (A) Coronal T2-weighted MR image shows pancreatoduodenal groove cystic lesions (white arrows), duodenum (black arrow) and normal pancreas (orange arrow). (B) Coronal thick-slab MR cholangiopancreatography image shows pancreatoduodenal groove cystic lesions and widening of the space between the distal pancreatic and common bile ducts and duodenal lumen (white arrow).
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
DUODENAL WALL THICKENING AND DUODENAL STENOSIS
Duodenal morphology can be identified on MRCP and cross-sectional images.
These studies also show and correlate this aspect with the tissue in the groove.
Typically,
in GP a thickened wall of the second portion of the duodenum is seen (Figure 6).
Duodenal evaluation is essential in differentiating GP from pancreatic cancer,
with the marked inflammatory duodenal wall thickening characteristic of GP and uncommon feature of pancreatic head tumors.

Fig. 6: (A) Axial T2-weighted MR image shows duodenal wall thickening (blue arrows) and cysts in duodenal wall and in pancreaticoduodenal groove (yellow arrows). (B) Thick-slab coronal MR cholangiopancreatography image reveal stenosis of descending duodenum (blue arrows).
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
COMMON BILE DUCT (CBD) TAPERING
Some degree of stenosis is virtually always present.
A long,
smooth segmental stenosis of the distal or intrapancreatic CBD or just a medial shift of the duct contracted by fibrosis can be observed in most patients.
This narrowing is typically smooth (Figure 7) unlike to the abrupt irregular ductal stricture or complete ductal obstruction seen in pancreatic cancers (Figure 8).
In some situations the stenosis leads to a mild retrograde biliary dilatation.
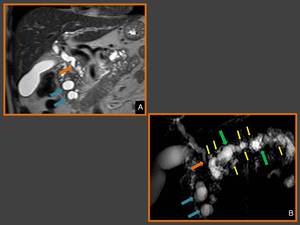
Fig. 7: (A) Coronal T2-weighted MR image and (B) thick-slab MR cholangiopancreatography image show common bile duct
tapering (arrows), which is typical of chronic pancreatitis, and cysts in the pancreaticoduodenal groove (blue arrows) . (B) Also shows dilation and tortuosity of main (green arrows) and secondary (yellow) pancreatic ducts.
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013

Fig. 8: Coronal 3D MR cholangiopancreatography image shows abrupt stenosis of the intrapancreatic portion of the bile duct (orange arrow), without identical grade of main pancreatic duct dilatation (white arrow), or duodenal cystic lesions, characteristic findings of groove adenocarcinoma.
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
PANCREATIC DUCT MORPHOLOGY
The main pancreatic duct (MPD) may appear normal in the pure form of GP,
but in the segmental form a stricture is usually seen as a mild,
regular,
and progressive narrowing within the pancreatic head associated with proximal dilatation.
This stricture or narrowing is usually longer than in cases of pancreatic adenocarcinoma,
while upstream dilatation in GP is not so marked.
In some patients,
higher degrees of dilation of the MPD and secondary duct ectasia can be seen (Figure 7 B),
these findings can be explained by the presence of both groove pancreatitis and diffuse chronic inflammatory disease.
MRCP with secretin stimulation demonstrates pancreas divisum and/or santorinicele,
which may be related due to impeded pancreatic outflow to the pathogenesis of GP.
WIDENING OF THE SPACE BETWEEN THE DISTAL PANCREATIC AND COMMON BILE DUCTS AND DUODENAL LUMEN ON MRCP
Widening of space between distal pancreatic and common bile ducts and duodenal lumen on MRCP is another sign not commonly seen in cases of pancreatic cancer,
but observed in most patients with GP.
This feature results from the combination of two factors: the presence of a space-occupying lesion in the pancreaticoduodenal groove and marked duodenal wall thickening (Figure 9).
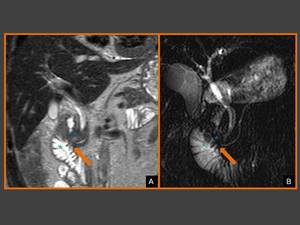
Fig. 9: (A) Coronal T2-weighted image and (B) coronal thick-slab MRCP image show widening of distance between duodenal lumen (green asterisk) and distal ducts (orange arrows) caused by inflammatory tissue in pancreaticoduodenal groove (blue asterisk).
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
BANANA-SHAPED GALLBLADDER
GP is not usually associated with a significant degree of biliary dilatation,
so the gallbladder tends to be normally distended.
A high prevalence of a banana-shaped gallbladder is detected on MRCP,
a sign frequently observed in chronic pancreatitis (Figure 10).
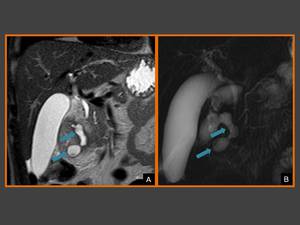
Fig. 10: (A) Coronal T2-weighted image and (B) coronal thick-slab MRCP image show banana-shaped gallbladder and the cysts in the pancreaticoduodenal groove (blue arrows).
References: Department of Radiology, Erasme Hospital, Libre University of Brussels/ Belgium 2013
